NAPLEX Asthma Practice Questions with Answers
Mastering NAPLEX asthma practice questions is essential for pharmacy candidates aiming to demonstrate proficiency in managing chronic respiratory conditions through pharmacological intervention and patient education. Asthma is a chronic inflammatory disorder of the airways characterized by variable and recurring symptoms, airflow obstruction, and bronchial hyperresponsiveness. To succeed on the exam, you must understand the latest Global Initiative for Asthma (GINA) guidelines, which emphasize the use of inhaled corticosteroids (ICS) even in mild disease to reduce the risk of exacerbations. Understanding the nuances of inhaler technique, step-up therapy, and drug-drug interactions is a core component of NAPLEX Prep.
Concept Explanation
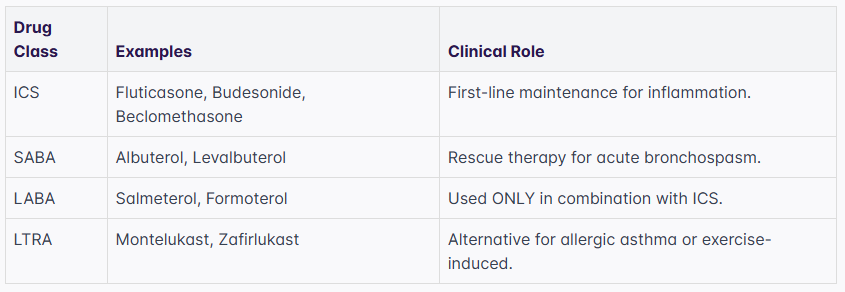
Asthma management focuses on achieving symptom control and minimizing the risk of future exacerbations through a stepwise pharmacological approach. The therapeutic regimen is divided into two main categories: controllers and relievers. Controllers, such as daily ICS, long-acting beta-2 agonists (LABA), and leukotriene receptor antagonists (LTRA), address the underlying airway inflammation. Relievers, traditionally short-acting beta-2 agonists (SABA) but now increasingly ICS-formoterol combinations, provide rapid relief during acute symptoms. Pharmacists must also be adept at interpreting pulmonary function tests, specifically the Forced Expiratory Volume in 1 second and the ratio, to assess the severity of obstruction. For more broad review, you may find the NAPLEX Respiratory Pharmacology Practice Questions helpful in solidifying these mechanisms of action.
Solved Examples
-
Determining Asthma Severity: A 24-year-old patient reports symptoms (cough, wheeze) 3 days per week and awakens at night due to asthma twice a month. Their is 85% of predicted. What is the severity classification?
-
Identify the frequency of daytime symptoms: 3 days/week fits "Mild Persistent" (defined as > 2 days/week but not daily).
-
Identify nighttime awakenings: 2 times/month fits "Mild Persistent" (defined as 3-4 times/month for adults).
-
Check lung function: FEV_1 > 80% is consistent with Mild Persistent asthma.
-
Conclusion: The patient has Mild Persistent asthma.
-
-
Calculating Peak Flow: A patient has a personal best Peak Expiratory Flow (PEF) of 400 L/min. During an episode, their current reading is 240 L/min. Which zone of the Asthma Action Plan are they in?
-
Calculate the percentage of personal best:
-
Recall the zone thresholds: Green (> 80%), Yellow (50-80%), Red (< 50%).
-
Conclusion: 60% falls into the Yellow Zone, indicating a need for caution and potential use of rescue medication.
-
-
Pharmacotherapy Selection: A patient is currently taking low-dose ICS but continues to have symptoms 5 days a week. What is the next preferred step in therapy according to GINA Track 1?
-
Identify the current step: The patient is on Step 2 (daily low-dose ICS).
-
Determine the next step (Step 3): The preferred controller is a low-dose ICS-formoterol combination as maintenance and reliever therapy (MART).
-
Conclusion: Switch to low-dose ICS-formoterol (e.g., Symbicort).
-
Practice Questions
-
Which of the following medications is associated with a Black Box Warning for serious neuropsychiatric events, including suicidal ideation?
-
A patient is prescribed Advair Diskus. What is the correct counseling point regarding the administration of this device?
-
Calculate the dose of Theophylline for a 70 kg patient using a target concentration of 10 mcg/mL and a volume of distribution () of 0.5 L/kg. What is the loading dose in mg?
Practice real clinical decision-making.
Improve therapeutic reasoning with pharmacy patient cases and scenario-based NAPLEX questions.
Practice Patient Cases-
A 12-year-old child presents with asthma symptoms daily and wakes up once every week. Their is 70% of predicted. Classify the severity.
-
Which asthma medication inhibits the 5-lipoxygenase enzyme to prevent leukotriene formation?
-
A patient is using a ProAir HFA inhaler. How should they be instructed to clean the plastic actuator?
-
What is the therapeutic range for Theophylline when used for the treatment of chronic asthma?
-
Which of the following monoclonal antibodies is specifically indicated for patients with severe asthma and an eosinophilic phenotype?
-
A patient is being switched from oral Prednisone 20 mg daily to an ICS. What is the primary reason for tapering the oral steroid rather than stopping it abruptly?
-
Which inhaler contains a dry powder and should not be shaken before use?
Answers & Explanations
-
Montelukast (Singulair): This LTRA carries a Boxed Warning for serious neuropsychiatric events. Patients and caregivers should be alerted to monitor for changes in behavior, aggression, or suicidal thoughts.
-
Advair Diskus (Fluticasone/Salmeterol): This is a Dry Powder Inhaler (DPI). The patient should breathe out fully (away from the device), place their lips firmly around the mouthpiece, and breathe in deeply and forcefully. They must rinse their mouth after use to prevent oral candidiasis.
-
Loading Dose Calculation: Using the formula , where . Therefore, .
-
Moderate Persistent Asthma: Daily symptoms and between 60-80% of predicted define Moderate Persistent asthma in children and adults.
-
Zileuton (Zyflo): Unlike Montelukast and Zafirlukast which are receptor antagonists, Zileuton inhibits the enzyme 5-lipoxygenase directly.
-
Cleaning HFA Inhalers: The plastic actuator of a SABA like ProAir HFA should be cleaned at least once a week by removing the canister and rinsing the actuator with warm running water, then air drying.
-
5-15 mcg/mL: The traditional range was 10-20, but for asthma management, a lower range of 5-15 mcg/mL is often targeted to minimize toxicity while maintaining efficacy.
-
Mepolizumab (Nucala), Reslizumab (Cinqair), or Benralizumab (Fasenra): These agents target Interleukin-5 (IL-5) or its receptor, which are key in eosinophilic inflammation.
-
Adrenal Insufficiency: Chronic use of systemic corticosteroids suppresses the Hypothalamic-Pituitary-Adrenal (HPA) axis. Abrupt withdrawal can lead to a life-threatening adrenal crisis.
-
Pulmicort Flexhaler or Spiriva Handihaler: Most DPIs (Diskus, Ellipta, Flexhaler) should not be shaken, as shaking can cause the loss of the metered dose.
1. Which medication is the preferred rescue inhaler for a patient on GINA Track 1 (MART) therapy?
Frequently Asked Questions
What is the difference between a MDI and a DPI?
A Metered-Dose Inhaler (MDI) uses a pressurized propellant to deliver a mist and requires coordination or a spacer, while a Dry Powder Inhaler (DPI) is breath-activated and requires a forceful, deep inhalation without shaking the device. You can learn more about inhaler techniques in our Hard NAPLEX Respiratory Pharmacology Practice Questions guide.
Why are LABAs not used as monotherapy in asthma?
LABAs used alone in asthma increase the risk of asthma-related deaths because they treat bronchodilation without addressing the underlying inflammation. They must always be used in combination with an inhaled corticosteroid (ICS) for safety. For similar safety profiles in other classes, see the NAPLEX Cardiovascular Pharmacology Practice Questions.
When should a patient use the "Yellow Zone" of their Asthma Action Plan?
The Yellow Zone is used when a patient's peak flow is between 50-80% of their personal best, indicating a worsening of symptoms that requires an increase in rescue medication or a temporary adjustment in maintenance therapy. Utilizing an AI Exam Simulator can help you practice these clinical scenarios.
What are the common side effects of inhaled corticosteroids?
Common local side effects of ICS include oral candidiasis (thrush), dysphonia (hoarseness), and cough, which can be mitigated by using a spacer and rinsing the mouth after administration. Systemic effects are minimal at standard doses but can include growth deceleration in children or decreased bone mineral density at very high doses.
How does Theophylline interact with Ciprofloxacin?
Ciprofloxacin is a potent inhibitor of CYP1A2, which is the primary enzyme responsible for metabolizing theophylline. Co-administration can significantly increase theophylline levels, leading to toxicity such as arrhythmias or seizures. This is a classic example of a drug interaction you might find in NAPLEX Pharmacology Practice Questions.
Is Xopenex (Levalbuterol) more effective than Albuterol?
Clinical studies generally show that levalbuterol (the R-isomer) offers no significant therapeutic advantage over racemic albuterol in terms of efficacy or reducing side effects like tachycardia at equivalent doses. It is often much more expensive, making it a second-line option based on cost-effectiveness.
Practice real clinical decision-making.
Improve therapeutic reasoning with pharmacy patient cases and scenario-based NAPLEX questions.
Practice Patient CasesTags
Enjoyed this article?
Share it with others who might find it helpful.